Treating Iron Deficiency With Ferric Carboxymaltose
Patent No. US11020369 (titled "Treating Iron Deficiency With Ferric Carboxymaltose") was filed by Pharmacosmos Holding As on Mar 18, 2020.
What is this patent about?
’369 is related to the field of treating iron deficiency with intravenous (IV) iron carbohydrate complexes, specifically ferric carboxymaltose (FCM). Iron deficiency impairs hemoglobin production, leading to fatigue and other symptoms. While oral iron is the first-line therapy, it often fails due to compliance issues and side effects. High-dose IV iron, like FCM, offers a rapid and effective alternative, but it can lead to side effects like hypophosphatemia (low serum phosphate).
The underlying idea behind ’369 is that FCM treatment, while effective for iron deficiency, can induce an auto-synergistic increase in iFGF23 (intact Fibroblast Growth Factor 23), a hormone that regulates phosphate and vitamin D. This increase can lead to reduced muscle function and increased bone turnover. The invention aims to mitigate these side effects by adjusting the timing and amount of FCM administered, selecting patients less likely to suffer from these side effects, monitoring patients after the first dose, and combining FCM with other drugs.
The claims of ’369 focus on methods of treating iron deficiency with FCM in subjects with a reduced risk for FGF23-mediated side effects. This involves administering a dose of 750mg of elemental iron followed by a further dose of 750mg of elemental iron, or a dose of 1000mg of elemental iron followed by a further dose in the range of 500mg to 1000mg of elemental iron. The claims also cover methods of monitoring subjects after a dose of FCM by measuring blood or urine parameters such as serum phosphate, vitamin D, ionized calcium, PTH, and urinary phosphate excretion to determine eligibility for a further dose. Additionally, the claims encompass methods for identifying subjects with a reduced risk for FGF23-mediated side effects based on these parameters, exclusion criteria, or respiratory capacity.
In practice, the invention involves a multi-faceted approach. First, patients are screened to determine their risk for FGF23-mediated side effects using blood tests, exclusion criteria (e.g., bariatric surgery, obesity, cardiac conditions), and respiratory capacity measurements. If a patient is deemed suitable, they receive an initial dose of FCM. Afterwards, their blood parameters are monitored to assess the impact on phosphate levels and other relevant markers. Based on these measurements, the timing and dosage of subsequent FCM administrations are adjusted to minimize the risk of adverse effects.
The differentiation from prior approaches lies in the recognition of the auto-synergistic effect of FCM on iFGF23 and the resulting clinical consequences. Previous studies considered FCM-associated hypophosphatemia to be transient and clinically irrelevant. ’369 challenges this view by providing methods for identifying at-risk patients, monitoring their response to FCM, and adjusting treatment regimens or using adjunctive therapies (like vitamin D or phosphate supplements) to mitigate the iFGF23-mediated side effects, thus optimizing the benefit-risk profile of FCM therapy. This proactive approach aims to prevent long-term complications like reduced muscle function and increased bone turnover.
How does this patent fit in bigger picture?
Technical landscape at the time
In the late 2010s when ’369 was filed, intravenous iron formulations were commonly used to treat iron deficiency, at a time when ferric carboxymaltose was a relatively new high-dose option allowing for faster iron correction compared to older, low-dose formulations. At this time, the potential for hypophosphatemia as a side effect of intravenous iron administration was recognized, but the clinical significance and long-term consequences were not fully understood, when systems commonly relied on serum phosphate measurements to monitor patients receiving intravenous iron, rather than routine monitoring of FGF23 levels or bone turnover markers.
Novelty and Inventive Step
The claims were rejected in a non-final Office action. The claims were rejected under 35 U.S.C. 112(b) or 35 U.S.C. 112 (pre-AIA), second paragraph, as being indefinite for failing to particularly point out and distinctly claim the subject matter which the inventor or a joint inventor regards as the invention. Claims 36-43 were rejected under 35 U.S.C. 112(d) or pre-AIA 35 U.S.C. 112, 4th paragraph, as being of improper dependent form for failing to further limit the subject matter of the claim upon which it depends. The prosecution record does NOT describe the technical reasoning or specific claim changes that led to allowance.
Claims
This patent contains 27 claims, with independent claims numbered 1, 6, and 10. The independent claims are directed to methods of treating iron deficiency with ferric carboxymaltose, methods of monitoring a subject who has been administered ferric carboxymaltose, and methods of identifying a subject having a reduced risk for FGF23-mediated side effects. The dependent claims generally add further details and limitations to the methods described in the independent claims.
Key Claim Terms New
Definitions of key terms used in the patent claims.
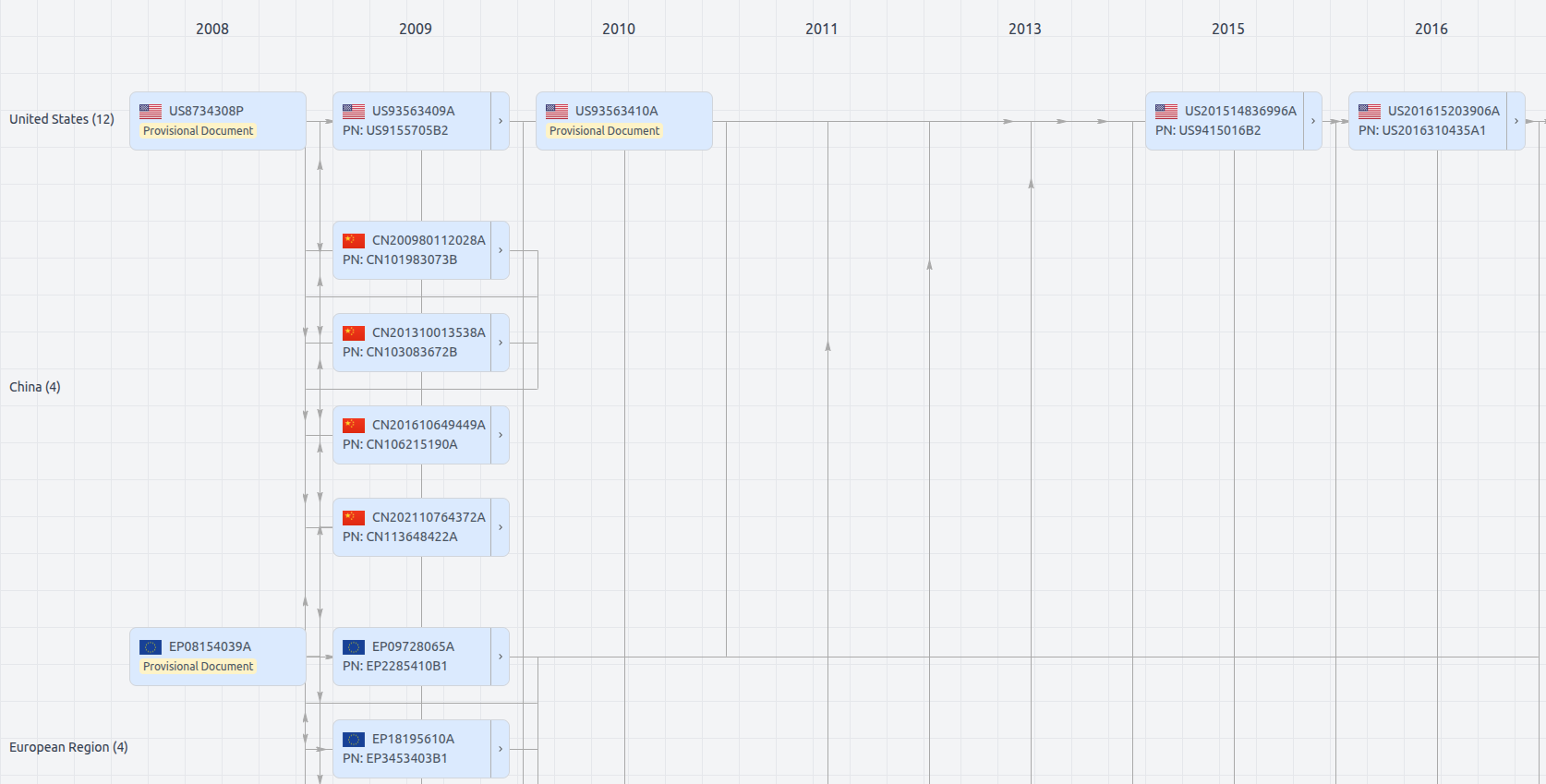
Patent Family
File Wrapper
The dossier documents provide a comprehensive record of the patent's prosecution history - including filings, correspondence, and decisions made by patent offices - and are crucial for understanding the patent's legal journey and any challenges it may have faced during examination.
Get instant alerts for new documents
US11020369
- Application Number
- US16822911
- Filing Date
- Mar 18, 2020
- Status
- Granted
- Expiry Date
- Oct 29, 2039
- External Links
- Slate, USPTO , Google Patents